
ކޮވިޑް-19 އަކީ ގައިން ގަޔަށް އަރާ ބައްޔެއް ހެއްޔެވެ؟
ގާނޫނު އަސާސީ ގައި އާންމު ސިއްހަތު ރައްކާތެރިކުރުމުގެ ގާނޫނުގެ ދަށުން އަސާސީ ހައްޤުތައް ހިފެހެއްޓޭނެ ގޮތް ކަމަށް ބުނެފައިވަނީ “ގައިންގަޔަށް އަރާފާނެ ބައްޔެއްގެ ސަބަބުން” ކަމުގަ އެވެ.
އާންމު ސިއްހަތު ރައްކާތެރިކުރުމުގެ ގާނޫނު (ގާނޫނު ނަންބަރ 7/2012) ގެ 3 ވަނަ މާއްދާ – ހައްގުތައް ހަނިކުރުން ގައި ބުނެފައިވަނީ “މި ގާނޫނުގެ ދަށުން ކުރާ ކަމެއްގެ ސަބަބުން، އެއްވެސް މީހެއްގެ މިނިވަންކަމަށް ނުވަތަ ހައްގަކަށް ހަނިކަމެއް ގެނެވޭނީ، ސިއްހީގޮތުން ނުރައްކާވެދާނެ ފަދަ ބަލިމަޑުކަމެއްގެ ސަބަބުން، ނުވަތަ ގައިންގަޔަށް އަރާފާނެ ބައްޔެއްގެ ސަބަބުން، ނުވަތަ ދުރާލާ އެންމެންނަށް އެނގި އޭގެން ރައްކާތެރިވާންޖެހޭފަދަ ބައްޔެއްގެ ސަބަބުން، ނުވަތަ އާންމު ސިއްހަތަށް ކުއްލި ނުރައްކަލުގެ ހާލަތެއް ދިމާވުމުގެ ސަބަބުން، ނުވަތަ އަމިއްލަ ސިއްހަތަށް ނުރައްކާވާފަދަ ކަމެއް ދިމާވުމުގެ ސަބަބުން، އެ ވަގުތަކަށާއި ހާލަތަކަށާއި ކަމުގެ ކުޑަބޮޑުމިނަށް ބަލާއިރު، މީހެއްގެ މިނިވަންކަމަށް ނުވަތަ ހައްގަށް ހަނިކަމެއް ގެންނަން ކޮންމެހެން ބޭނުންވާ މިންވަރަށް، މި ގާނޫނުގެ ދާއިރާގެ ތެރޭގައި ހަމައެކަނި އެ ނިސްބަތަށެވެ.”
އަދި މި ޤާނޫނުގައި ބަޔާންކޮށްފައިވަނީ ގައިން ގަޔަށް އަރާ ބަލި ބަޔާންކުރަން ޖެހޭނީ “ސާބިތުވާންހުރި ސިއްހީ އިލްމާއި ހޯދުންތަކުގެ އަލީގައި” ކަމުގައި ވަނީ ބަޔާންކޮށްފަ އެވެ. އެހެންކަމުން، ބައްޔެއް ގައިން ގަޔަށް އަރަންޏާ އެކަން ސާބިތުވާންހުރި ސިއްހީ އިލްމަމާއި ހޯދުމެއް އޮންނަން ޖެހޭނެ އެވެ.
ދެންނެވި ޤާނޫނުގެ “11 ވަނަ މާއްދާ – ގައިންގަޔަށް އަރާ ބަލި ބަޔާންކުރުން (ހ) ސާބިތުވާންހުރި ސިއްހީ އިލްމާއި ހޯދުންތަކުގެ އަލީގައާއި، ލިބިފައިވާ މާޒީގެ ތަޖުރިބާގެ އަލީގައާއި، ބައިނަލްއަގްވާމީ ހަމަތަކާއި އުސޫލުތަކުގެ އަލީގައި، ގައިންގަޔަށް އަރާ ބަލިކަމަށް މި ގާނޫނުގެ ދަށުން ބަލާނެ ބަލިތައް، މި ގާނޫނުގެ ދަށުން ހަދާ ގަވާއިދުގައި ބަޔާންކުރަންވާނެއެވެ. އަދި (ށ) ގައިންގަޔަށް އަރާ ބަލިތަކަކީ ކޮބައިކަން، މި މާއްދާގެ (ހ) ގައިވާ ގޮތުގެމަތިން، މި ގާނޫނުގެ ދަށުން ހަދާ ގަވާއިދުގައި ބަޔާންކުރުމުގެ އިތުރަށް، ސާބިތުވާންހުރި ސިއްހީ އިލްމާއި ހޯދުންތަކުގެ އަލީގައާއި، ބައިނަލްއަގްވާމީ ހަމަތަކާއި އުސޫލުތަކުގެ އަލީގައާއި، ލިބިފައިވާ މާޒީގެ ތަޖުރިބާގެ އަލީގައި، ވަކި ބައްޔެއް އެއީ ގައިންގަޔަށް އަރާ ބައްޔެއްކަމަށް ކަނޑައަޅާނެ އާންމު އުސޫލުތައްވެސް، މި ގާނޫނުގެ ދަށުން ހަދާ ގަވާއިދުގައި ބަޔާންކުރަންވާނެއެވެ.”
ކޮވިޑް-19 އާއި ގުޅުވައިގެން ދިވެހި ރައްޔިތުންނަށް ދީފައިވާ އަސާސީ ހައްޤުތައް ހިފެހެއްޓައި މި ޤާނޫގައި ދީފައިވާ ބާރުތަކުން އެކިއެކި ފިޔަވަޅުތައް އެޅައި ކަންކަން ކުރެވޭނީ އެއީ ގައިން ގަޔަށް އަރާ ބައްޔެއް ކަމުގެ ސާބިތު ހެކި އޮވެގެން ނެވެ. އެ ނެތި ބަޔަކު ޞިއްޙީ ގޮތުން އީމާންވެ ޤަބޫލުކުރާ ޤަބޫލު ކުރުންތަކުގެ މައްޗަށް ހައްޤުތައް ހިފެހެއްޓުމުގެ ހައްޤެއް ޤާނޫން އަސާސީން އެއްވެސް މީހަކަށް ބާރު ދީފައި ނުވެ އެވެ.
ކޮވިޑް-19 ގެ ހަޤީޤަތުގެ މައްޗަށް ބަލާލުމެއް
ޢާންމު ތަޢުރީފުތައް:
ސާރސްކޮވް-2: ކޮވިޑް-19 ބަލި ޖައްސާކަމުގައި ދަޢުވާކުރާ ވައިރަސް.
ކޮވިޑް-19: ސާރސްކޮވް-2 ކިޔާ ވައިރަސް އަކުން ޖެހޭ ކަމުގައި ކިޔާ ބަލި، ބަލީގެ ތަޢުރީފް ހަޤީޤަތުގައި ސާފެއް ނޫން. ބަލި ޖެހިފައިކަމަށް ބަލަނީ ޢާލާމާތްތަކަށްވުރެ ބޮޑަށް ލެބޯޓްރީގައި ހަދާ ޑީއެންއޭ އާރްއެންއޭ އުފައްދައި ގިނަކުރާ ޓެސްޓަކަށް.
ކޮވިޑް-19 ގެ ޢަލާމާތްތައް: ސާސްކޮވް އިން ޖެހޭ ޢަލާމާތްތައް ގޮތުގައި ބުނެފައިވާ ކަންކަމުގައި ހިމެނެނީ ރޯގާ ޖެހުމާއި، ހުން އައުމާއި، ނޭވާލާން އުނދަގޫވުމާއި، ކެއްސުމާއި، ވަރުބަލިވުމާއި، މަސްތަކަށް ތަދުވުމާއި، ބޮލުގައި ރިއްސުމާއި، ރަހަ ކެނޑުމާއި، ބޭރަށް ހިނުމާއި، ހޮޑުލެވުމާއި، މޭނުބައިކުރުމާއި، ބޮލުގައި ރިއްސުމާއި ވަރުބަލިވުމާއި، އަދި ނިއުމޯނިއާ ފަދަ ކަންކަމެވެ. މިކަންކަމަކީ އެބުނާ ސާރސްކޮވް-2 ކިޔާ ވައިރަސް އިން ޖައްސާ ކަމުގެ ފަންނީ އެއްވެސް ހެއްކެއް އެބަ އޮތް ހެއްޔެވެ؟ ނެތެވެ.
30 ޖޫން 2020: މި ތާރީޚްގައި އެޗްޕީއޭ އިން ނެރެފައިވާ ”ކޮވިޑް-19 ރެފަރެންސް ގައިޑް“ ގައި ބުނެފައި ވަނީ”(ކޮވިޑް-19) ކޮރޯނާވައިރަސް ބައްޔަކީ ސިވިއާ އެކިއުޓް ރެސްޕިރޭޓަރީ ސިންޑްރޮމް ކޮރޯނާ ވައިރަސް2 (ސާސް-ކޮވް-2) އިން ޖެހޭ ބައްޔެކެވެ. މި އާ ކޮރޯނާ ވައިރަސް އެންމެ ފުރަތަމަ އައިޑެންޓިފައި ކުރެވިފައިވަނީ، ޗައިނާގެ ހުބެއި ޕްރޮވިންސުގެ ވޫހާން ސިޓީ އިންނެވެ. މީގެ ވާހަކަ އެންމެ ފުރަތަމަ ޑަބްލިއުއެޗްއޯއަށް ރިޕޯޓު ކުރެވުނީ 31 ޑިސެންބަރ 2019 ގަ އެވެ. ޗައިނާގެ ރަސްމީ އިދާރާތަކުން ވައިރަސް އައިސޮލޭޓްކުރީ (ވަކިކުރީ) 7 ޖެނުއަރީ 2020 ގައެވެ. ކޮވިޑް-19 ބަލިމަޑުކަން ފެތުރުމަކީ ގްލޯބަލް ހެލްތު އެމެޖިންސީއެއް ކަމުގައި ޑަބްލިއުއެޗްއޯއިން އިއުލާނުކުރީ 30 ޖެނުއަރީ 2020 ގައެވެ. 11 މާޗް 2020 ގައި ކޮވިޑް-19 އަކީ ގްލޯބަލް ޕެޑަމިކެއް ކަމުގައި ޑަބްލިއުއެޗްއޯ އިން އިއުލާނު ކުރި އެވެ.”
ސިޔާސީ އަދި މާލީ އިޤްތިޞާދީ މަސްލަހަތު ޙިމާޔަތްކުރުމަށް ސައިންސު ބޭނުންކުރަމުން ދަނީ!
13 ނޮވެންބަރު 2020 ގައި ބީއެމްޖޭ ޖާނަލްގައި “ކޮވިޑް-19: ސިޔާސީކުރުން “ކޮރަޕްޝަން” އަދި ސައިންސު ގަދަކަމުން ހުއްޓުވުން” މި މައުޟޫއަށް ލިޔެފައިވާ ފާހަގަކޮށްލެވޭ އެޑިޓޯރިއަލް ގައި ބުނެފައިވެ އެވެ. “ފައިސާގެ ބޭނުންތަކާއި ސިޔާސީ އެދުންތަކަށް ސައިންސް ދަނީ ގަދަކަމުން ހުއްޓުވާ ލެވެމުން ނެވެ. ކޮވިޑް-19 އިންވަނީ އިންތިހާއަށް ބޮޑު މިނެއްގައި ސްޓޭޓް ކޮރަޕްޝަން ނެރެ ދީފައެވެ. މެޑިކަލް އަދި ސިޔާސީ ގުޅުމުގެ ނިޒާމުން ސައިންސު ހުއްޓުވުމާއި ދިމާއަށް ގޮސްފައިވަނީ ބާރުތަކުގެ މަތީގައިވާ މީހުން އިތުރަށް މުއްސަނދިކޮށް ބާރުވެރި ކުރުމަށެވެ. އަދި ދުނިޔޭގެ ބާރުވެރިން ކާމިޔާބުވެ މުއްސަނދިވާ ވާވަރަކަށް، އެމީހުން ބާރުގެ މައްޗަށް މަސްތުވެ، ސައިންސުގެ ހަޤީޤަތްތައް ފޮރުވައި ހުއްޓުވާނެ އެވެ. ރަނގަޅު ސައިންސު ހުއްޓުވަމުން ގެންދިއުމުން މީހުން މަރުވެ އެވެ.”
“Science is being suppressed for political and financial gain. Covid-19 has unleashed state corruption on a grand scale, and it is harmful to public health. The medical-political complex tends towards suppression of science to aggrandize and enrich those in power. And, as the powerful become more successful, richer, and further intoxicated with power, the inconvenient truths of science are suppressed. When good science is suppressed, people die.”[1]
މިފަދަ އޮޅުވާލުމާއި ހީލަތްތެރި މަކަރުވެރިކަން ފެނިގެން ދިޔަ އެއް ގައުމަކީ ކޮމިއުނިސްޓް ޗައިނާ އެވެ. އެތަނުގެ ރައްޔިތުން އެއާ ޕޮލިއުޝަން އާއި ދެކޮޅަށް މުޒާހަރާ ކުރަން ފެއްޓުމުން އެމީހުން އެކަން ފޮރުވައި ވަޅުޖަހަން އެމީހުން ޖެހި ރޮކެޓަކީ އައު ވައިރަސް އެއް ނުކުމެގެން އުޅޭ ދޮގުވެރި ވާހަކަ އެވެ.
ދައްކަން ބޭނުންނުވާ ވާހަކަ: ޗައިނާގެ އެއާ ޕޮލިއުޝަންގެ ސަބަބުން އާންމު ޞިއްހަތަށް އޮތް ނުރައްކާ
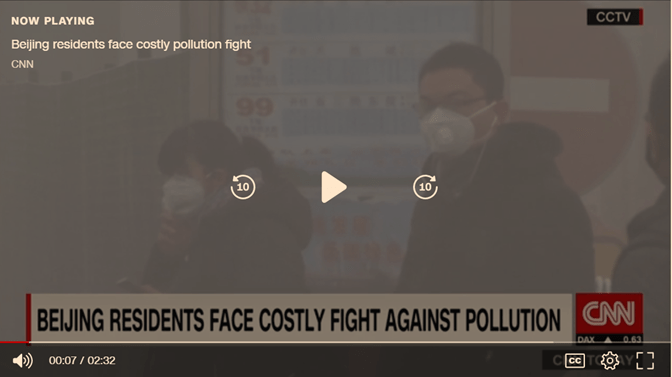
7 ޖުލައި 2019: އެއާ ޕޮލިއުޝަންއާއި ދެކޮޅަށް ޗައިނާގެ ބެއިޖިން އިން ފެށިގެން އައި މުޒާހަރާ ވޫހާން ސިޓީގައި ކުރެވުމެވެ.[2] މިއީ ތާރީޚުގެ ތެރެއިން ހަނދާނުން ފޮހެލާފައި ވާ ވާހަކަތަކުގެ ތެރެއިން މުހިންމު އެއް ވާހަކަ އެވެ. މަތީގައިވާ ފޮޓޯގައި އެފެންނަނީ އެއާ ޕޮލިއުޝަންގެ ބޮޑުކަމުން އޭރުވެސް ބަޔަކު ޗައިނާގެ ސިޓީގައި މާސްކު އަޅައިގެން އުޅޭ މަންޒަރެވެ. [3] އެއާ ޕޮލިއުޝަންގެ ސަބަބުން ކޮންމެ އަހަރަކު 7 މިލިއަން މީހުން މަރުވާ ކަމުގައި ޑަބްލިޔުއެޗްއޯ އިން ބުނެ އެވެ. އެހެނަސް، މިކަން އެއްވެސް ކަމަކަށް ނުވެ އެވެ. އެއާ ޕޮލިއުޝަން އަކީ ފުއްޕާމޭގެ އެކި ބަލިތައް މެދުވެރިވުމުގެ އެންމެ ބޮޑު އަސްލެވެ. އެހެނަސް، ޗައިނާގެ ވެރިންނަށް މިކަން ކަމަކަށް ނުވި އެވެ. އެހެނަސް، އެމީހުން މުޖްތަމަޢަށް ދޫކުރީ ޚިޔާލީ ވައިރަސް އެއްގެ ސްޓޯރީ އެކެވެ. ނޮވެލް ކޮރޯނާ ވައިރަސް އެއްގެ ވާހަކަ އެވެ.
ސާރސްކޮވް ވައިރަސް އައިސޮލޭޝަން:
ފުރިހަމަ ގޮތުގައި އައިސޮލޭޓް ކުރެވިފައިވާ ކޮރޯނާ ވައިރަސް އެއް ދައްކައި، އެއިން ބައްޔެއް ޖައްސާ ކަން ސާބިތުކޮށްދީފިނަމަ 100000 ޑޮލަރު ދޭނަން – ޑރ. ތޯމަސް ކޮވަން
ސުވާލަކީ ސާރސްކޮވް-2 ވައިރަސް އައިސޮލޭޓްކޮށް ހޯދާފައިވޭތޯ އަދި އެއިން ބަލި (އެބުނާ ޢަލާމާތްތައް) ޖައްސާކަން ސާބިތުކޮށްފައިވޭތޯ އެވެ؟
އެމެރިކާގެ ސީޑީސީ: ކޮވިޑް ވައިރަސް އައިސޮލޭޓް އެއް ނެތް ކަމުގައި ބުނެފައިވޭ
13 ޖުލައި 2020: ޕީސީއާރު ޓެސްޓު ވެލިޑޭޓް ކުރުމަށް “ކުއެންޓިފައިޑް ވައިރަސް އައިސޮލޭޓް ނެތް” ކަމުގައި އެމެރިކާގެ ސީޑީސީ އިންވަނީ އެމީހުން ނެރުނު ލިޔުމުގައި ބަޔާންކޮށްފަ އެވެ.
ޗައިނާގެ ސީޑީސީ: ކޮވިޑް ވައިރަސް އައިސޮލޭޓްކޮށްފައިނުވޭ
24 ޖެނުއަރީ 2021: މމި ދުވަހުގައި އެންބީސީ ނިއުސް ރިޕޯޓާ ޖެނިސް މެކީ ފްރެޔާ، ޗައިނާގެ ސެންޓާރ ފޯ ޑިސީސް ކޮންޓްރޯގެ ޗީފް އެޕިޑިމިއޮލޮޖިސްޓެއް ކަމުގައިވާ ޑރ. ވޫ ޒުންޔޯ ކައިރިން މީގެ އަހަރެއް ހާ ދުވަސް ކުރިން ނެގި ސާމްޕަލް އާއި ބެހޭ ޑޭޓާ ހިއްސާ ނުކުރެއްވީ ކީއްވެތޯ ސުވާލުކުރުމުން އޭނާ ޖަވާބުގައި ވިދާޅުވީ ވައިރަސް އައިސޮލޭޓް ނުކުރާތީވެ ކަމުގަ އެވެ. “އެމީހުން ވައިރަސް އައިސޮލޭޓް ކޮށްފައި ނުވެއެވެ. މައްސަލައަކީ އެއީ އެވެ.” އޭނާއާއި އަނެއްކާ ސުވާލު ކުރެވުނެވެ. “ދިރިހުރި ޖަނަވާރުގެ ސާލްޕަލް އާއި މެދު ބުނަނީ ކީކޭ ތޯ؟” ސުވާލު ކުރުމުން ޖަވާބުގައި ޑރ. ވޫ ޒުންޔޯ ވިދާޅުވީ “އެއިން އެއްވެސް އެއްޗެއް ކަލެއަށް ބުނަ ނުދޭނެ އެވެ. އޭތި އައިސްގެން އުޅެނީ އަހަރެމެން ކުރިން ހީކުރިގޮތަށް ކަމުގައި މިހާރު އަހަރެން ނުދެކެމެވެ.” [4]
ކޮވިޑް ވައިރަސް އައިސޮލޭޓްކޮށްފައި ވާކަމަށް ނެރެފައިވާ އެންމެހާ ޕޭޕަރުތަކަކީ ސޫޑޯ-ސައިންސް ފޭކު ދޮގުވެރު މަކަރުވެރި ޕޭޕަރު:
ތެދެކެވެ. ކޮވިޑް-19 ވައިރަސް އައިސޮލޭޓް ކޮށްފައިވާ ކަމަށް އެކި އެކި ފަރާތްތައް އެކިއެކި ދިރާސާތައް ދައްކާ ހަދަ އެވެ. އެހެނަސް، އޭގައި ވަނީ ދޮގެކެވެ. “ޖާނަލް ތަކުގައި ރިސާޗުތަކުގެ ގޮތުގައި ނެރެފައިވާ ގިނަ ދިރާސާތަކަކީ ދޮގުވެރި ދިރާސާތަކެއް” ކަމުގައި ސްޓޭންފޯޑް ޔުނިވާސިޓީގެ ޕްރޮފެސަރ އޮފް މެޑިސިން އަދި ޕްރޮފެސަރ އޮފް އެޕިޑެމިއޮލޮޖީ އެންޑް ޕޮޕިއުލޭޝަން ހެލްތުގެ މަޝްހުރު ޑޮކްޓަރު، ޑރ. ޖޯން އައޮނިޑިސް ވަނީ ވިދާޅުވެފަ އެވެ.[5] އެހެންކަމުން، ފަންނީ ދިރާސާއެއް ފެންނަ އިރަށް އެ ދިރާސާއެއް ކިޔަން ޖެހޭނީ އޭގެ ބުނާ ވާހަކަތަކާމެދު ދެކޮޅުން ވިސްނައި އޭގެ ތެދުދޮގު ބަލާ އުޞޫލަކުން ނެވެ. ތަނެއްގައި ދިރާސާއެއް ނެރެފައި އޮތުމަކީ އަދި އެއީ ތެދު އެއްޗަކަށް ވުމެއް ނޫނެވެ.

2019 ވަނަ އަހަރުން ފެށިގެން ކަން ހިނގައިދިޔަ ގޮތް:
12 ޑިސެންބަރ 2019: ޗައިނާގެ ވޫހާން ސިޓީގެ މާރުކޭޓާއި ގުޅުން އޮތް 198 މީހުންނަށް ބައްޔެއް ދިމާވެގެން އުޅޭ ކަމުގައި ބުންޏެވެ. އަދި 20 ޖެނުއަރީ ހަމައަށް އައި އިރު އޭގެ ތެރެއިން 3 މީހުން މަރުވި އެވެ. ބާކީތިބި އެންމެން ރިކަވާވި އެވެ. މި މީހުންނަކީ ގޮތް ނޭނގޭ ނިއުމޯނިއާ އެއް ޖެހިފައިވާ ބައެއް ކަމުގައި ވަނީ ދަޢުވާ ކޮށްފައެވެ. އެހެނަސް، ގޮތް ނޭނގޭ ނިއުމޯނިއާ އެކޭ ބުނީ ކީއްވެ ހެއްޔެވެ. ޗައިނާ އަކީ ނިއުމޯނިއާއާއި ކޮންމެ އަހަރަކު އެތައް މިލިއަން ބައެއް މަރުވާ ތަނެކެވެ. ކުރިންވެސް ބުނި ފަދައިން ޗައިނާގެ ވޫހާން ސިޓީއަކީ އިންތިހާއަށް އެއާ ޕޮލިއުޝަން ބޮޑު ސިޓީއެކެވެ. އެއާ ޕޮލިއުޝަން އަކީ ނިއުމޯނިއާގެ ބޮޑު އެއް އަޞްލެވެ.
ނިއުމޯނިއާ އަކީ ނޭވާލާ ގުނަވަން ކަމުގައިވާ ފުއްޕާމެއަށް ލިބޭ އަނިޔާ ނުވަތަ އިންފެކްޝަން އަށް ކިޔާ ޢާންމު ނަމެކެވެ. ފުއްޕާމެއަށް އަނިޔާވުމުގެ ސަބަބުން ފުއްޕާމޭގައި ދޮސްހެދި ފެން ހެދޭގޮތް ވެއެވެ. ނިއުމޯނިއާ އަކީ ވަރަށް ބައިވަރު ސަބަބުތަކުން މެދުވެރިވާ ކަމެކެވެ. ހަމައެކަނި މީހާ މުސްކުޅިވުމުން ވެސް ނިއުމޯނިއާ ޖެހިދާނެ އެވެ. ފުއްޕާމޭގައި ފެން ހެދިދާނެ އެވެ. ހޮސްޕިޓަލުން ދޭ ފަރުވާއެއްގެ ސަބަބުންވެސް ފުއްޕާމެއަށް ނިއުމޯނިއާ ޖެހެ އެވެ. އެއަށް ކިޔަނީ ހޮސްޕިޓަލް އެކުއާޑް ނިއުމޯނިއާ އެވެ. މިސާލަށް ވެންޓިލޭޓަރަށް ލާން ނުޖެހޭ މީހުން ހޭނައްތައި ވެންޓިލޭޓަރ އަށް ލުމުގެ ސަބަބުން ފުއްޕާމެއަށް ލިބޭ އަނިޔާއެއްގެ ސަބަބުން ނިއުމޯނިއާ ޖެހެ އެވެ. ފުއްޕާމެއަށް ދިޔާއެއްޗެއް އެޅުމުގެ ސަބަބުން ނިއުމޯނިއާ ޖެހިދާނެ އެވެ. ވައި ނުސާފުކަމުން ނުވަތަ ނޭވާލެވޭ ވިހަ ޓޮކްސިކް ކެމިކަލް އެއްގެ ސަބަބުން ނިއުމޯނިއާ ޖެހިދާނެ އެވެ. އެހެނަސް، މިއިން އެއްވެސް ކަމެއް އެމީހުންނަކަށް މުހިންމު ކަމަކަށް ނުވި އެވެ.
ޑަބްލިޔުއެޗްއޯއިން މި ވާހަކަ ރިޕޯޓްކުރުން
31 ޑިސެންބަރ 2019: ގޮތް ނޭނގޭ ނިއުމޯނިއާގެ ކޭސްތަކެއް ޗައިނާގެ ވޫހާން ސިޓީގައި ފެނިގެން އުޅޭ ކަމުގައި ޑަބްލިޔުއެޗްއޯއަށް އެންގި ކަމުގައި އެފަރާތުން ބުނެފައިވެ އެވެ.
7 ޖެނުއަރީ 2020: މި ތާރީޚުގައި އައު ކޮރޯނާ ވައިރަސް އެއް ޗައިނާގެ ވެރިން ތައް (އެބަހީ ޗައިނާގެ ސީސީޑީސީ އިން) ހޯދާފައި (އައިޑެންޓިފައި) ކޮށްފައި ވާކަމުގައި ޑަބްލިޔު އެޗްއޯއިން ވަނީ ދަޢުވާ ކޮށްފައެވެ. އެ ހޯދި ކަމަށް ދަޢުވާކުރި އެއްޗަށް އެމީހުން ވަގުތީ ގޮތުން ދިން ނަމަކީ 2019 އިގެ އައު ކޮރޯނާ ވައިރަސް (2019-nCoV) އެވެ. މި ހޯދުމުގައި އެންމެ އިސް ރޯލެއް އަދާކޮށްފައިވަނީ ވޫހާން އިންސްޓިޓިއުޓް އޮފް ވައިރޯލޮޖީ، ޗައިނާގެ ހުބެއި ޕްރޮވިންސްގެ ސެންޓާ ފޯ ޑިސީސް ކޮންޓްރޯލް (ސީޑީސީ) އެވެ. އެމީހުން ބައިވެރިވުމާއެކު ވައިރަސް ހޯދާފައިވާކަމަށް ތައްޔާރުކޮށްފައިވާ ޕޭޕަރުތައް ޢާންމުނަށް ފެންނަ ހިސާބަށް ނެރެފައި ވަނީ 23 ޖެނުއަރީ އަދި 24 ޖެނުއަރީ ގައެވެ. އެހެނަސް، އެބުނާ އާރްއެންއޭ އިން އެމީހުންނަށް ނިއުމޯނިއާ ޖެއްސިކަން ސާބިތުކޮށްފައި ނުވެ އެވެ.
އައު ވައިރަސް އެއް ހޯދާފައިވާ ކަމަށް ނެރެފައިވާ އެންމެ ފުރަތަމަ ޕޭޕަރު:
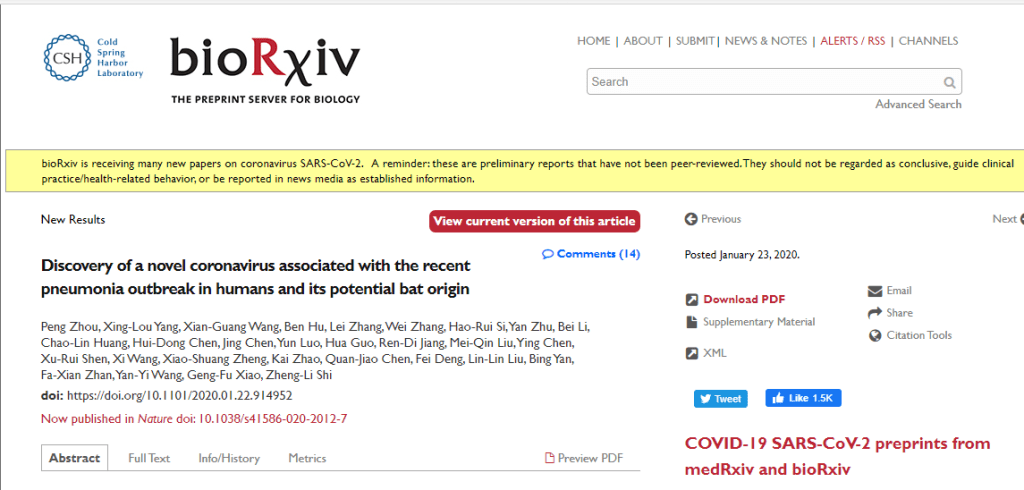
23 ޖެނުއަރީ 2020 ގެ ޕޭޕަރު: ވައިރަސް ހޯދާފައިވާ ކަމަށް ނެރެފައިވާ ފުރަތަމަ ދިރާސާ ނެރެފައިވަނީ ނިއު އިންގްލެންޑް ޖާނަލް އޮފް މެޑިސިން ގައި “ޑިސްކަވަރީ އޮފް ނޮވެލް ކޮރޯނާވައިރަސް އެސޯސިއޭޓެޑް ވިތް ދަ ރީސެންޓް ނިއުމޯނިއާ އައުޓްބްރޭކް އިން ހުމަން އެންޑް އިޓްސް ބެޓް އޮރިޖިން” [6] މި ނަމުގަ އެވެ.
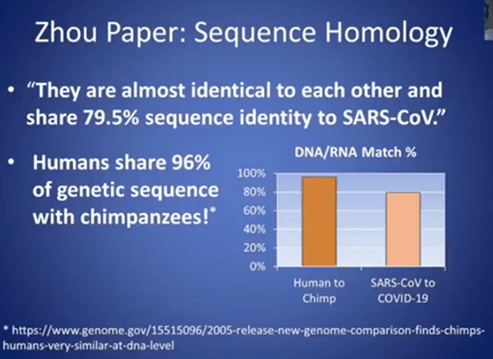
މި ޕޭޕަރުގައި ބަޔާންކޮށްފައިވާ ގޮތުން އެމީހުން ފެނުނު ކަމުގައި ބުނި އެއްޗަކީ ކޮރޯނާ ގެ އައު ވައިރަސް އަކަށް ނިންމީ ސާސް-ކޮވް އާއި %79.5 ޕަސެންޓު ދިމާވާތީ އެވެ.
79.5% sequence identify to SARS-CoV
މި ބުނެވޭ “ވައިރަސް” އޭ ކިޔާ ޖެނެޓިކް މާއްދާ އަކީ ކޮރޯނާ “ވައިރަސް”ގެ ބާވަތެއް ކަމުގައި ނިންމާފައިވަނީ އެ ބުނާ ސާމްޕަލުން ނެގި ދިޔައިގައި ހުރި އެއްޗެއްގެ ޖެނެޓިކް ސީކުއެންސާއި ކުރިން ކޮރޯނާ ކިޔާފައި ހޯދައިގެން އުޅޭ އެއްޗަކާއި ގާތްގަޑަކަށް %80 ވައްތަރު ވާތީ އެވެ.
ޑރ. އެންޑްރިއު ކައުފްމަން މި ކަމުގެ މައްޗަށް ވިދާޅުވެފައިވަނީ “މިހާރު އެމީހުން ހޯދައިގެން އުޅޭ އެއްޗަކީ ކޮރޯނާ ވައިރަސް އެކޭ ބުނެފައިވަނީ ކުރިން ހޯދުނު އެއްޗާއި %80 އާރްއެންއޭ ސީކުއެންސް އަޑެންޓިޓީ ދިމާވާތީ. އެހެނަސް، އަހަރެމެން އިންސާނުންނާއި މަކުނުގެ ބާވަތެއް ކަމުގައިވާ ޗިންޕަންޒީ އަކީ ތަފާތު ދެ ދިރުމުގެ ބާވަތެއްކަމުގައި ވާއިރުވެސް، މަކުނާއި އިންސާނުގެ ޖެނެޓިކް ސީކުއެންސު އައިޑެންޓިޓީ %97 އެއްގޮތް ކަމެއް ހުރޭ. މިފަދަ ދަށް ޕަސެންޓޭޖަކުން އެއީ އާ ކޮރޯނާ ވައިރަސްއެއް ކަމުގައި ނިންމި ގޮތް އަހަރެންނަށް ފަހުމެއް ނުވޭ.”
ވައިރަސް ފުރިހަމައަށް އައިސޮލޭޓް ކުރިތަ؟
- މި މީހުން ވައިރަސް އެއް އައިސޮލޭޓް ނުކުރޭ، ހަމައެކަނި ޖެނެޓިކް މެޓީރިއަލް ތަކެއް ނެގީ
- ހޯސްޓު ސެލްގައި ކަލްޓިވޭޓް (ދިރުވައި އާލާ) ނުކުރޭ، އޭގެ ބަދަލުގައި ކުރީ (ވީރޯ ސެލްސް އަދި އެޗްޔޫއެޗް 7 ސެލްތައް” އެއީވެސް 7 މީހުންގެ ތެރެއިން 1 ކަކަށް.
- ފިލްޓަރބިލިޓިއެއް ވެސް ސާބިތުކޮށްފަ ނެތް
މި ދިރާސާގައި ބުނެފައިވަނީ ޗައިނާގެ ވޫހާންގައި އެކިއުޓް ރެސްޕަރޭޓަރީ ސިންޑްރޯމް (ކުއްލިއަކަށް ފުއްޕާމެއަށް ޖެހުނު ބަލި) ޖެހުމަށް މެދުވެރިވި ކަމުގައި ގާތްކުރާ (ދި ލައިކްލީ) އިޓިއޮލޮޖީ (ސަބަބުކަމުގައިވާ) އެޖެންޓަކީ (އެއްޗަކީ) އެންކޮވް-2019 ކަމުގެ މައްޗަށް ތަފްޞީލީ ރިޕޯޓެއް އެކުލެވޭ ދިރާސާ އެއް ކަމުގަ އެވެ. މީގައި އެމީހު ބުނެފައިވަނީ ބަލި ޖެހުމަށް ގާތްކުރާ (ލައިކްލީ) އެއްޗަކީ އެއީ ކަމުގަ އެވެ. އެމީހުންނަށް ޔަޤީނެއް ވެސް ނޫނެވެ. ދެވަނައަށް ބުނެފައިވަނީ މި ބައްޔާއި މި ވައިރަސް (ކިޔާ މާއްދާ) އެމީހުންގެ ހަށިގަނޑުގައި ވުމާއި ގުޅުމެއް (ގާތް ކަމެއް، އެސޯޝިއޭޝަން އެއް) ދެމެދުގައިވާ ކަމަށެވެ. ގުޅުމެއް އަދި ގާތްކަމެއް ވުމަކީ ކަން ދިމާވާން މެދުވެރިވި ސަބަބު ކަމުގައި ނުވެދާނެ އެވެ. އަދި އޭގެ އިތުރަށް ބުނެފައިވަނީ މި ދިރާސާ ނެރޭ އިރުވެސް ކޮންމެހެން ޖަވާބު ލިބެންޖެހޭ ގިނަ ސުވާލުތައް ވާކަމުގައި ބުނެފައިވެ އެވެ. އޭގެ މާނައަކީ ހަޤީޤަތުގައި ވައިރަސް އިން ބަލި ޖައްސާ ކަން ޔަޤީން ވާވަރަށް މައުލޫމާތު ނެތް ކަމެވެ. އަދި އޭގެ އިތުރަށް ބުނެފައިވަނީ ހަމަ ހަޤީޤަތުގައި ވެސް މި ބުނާ ވައިރަސް އަކީ ބަލި ޖެހުމަށް މެދުވެރިވި ސަބަބު ކަމުގައި ކޮންފާމް ކޮށް ޔަޤީންކުރުމަށް އަދި ބަލި ޖެހިފައިވާ މީހުންގެ އިތުރު ގިނަ ޑޭޓާ އާއި ސާމްޕަލްތައް އެ މީހުން ބޭނުންވާ ކަމުގަ އެވެ.
The study provides the first detailed report on nCoV-2019, the likely etiology agent responsible for ongoing acute respiratory syndrome epidemic in Wuhan, central China. ….. The study provides …… provides evidence of an association between the disease and the presence of this virus. However, there are still many urgent questions to be answered. We need more clinical data and samples to confirm if this virus is indeed the etiology agent for this epidemic..
24 ޖެނުއަރީ 2020 ގެ ޕޭޕަރު: ވައިރަސް ހޯދާފައިވާ ކަމަށް ނެރެފައިވާ ފުރަތަމަ ދިރާސާ ނެރެފައިވަނީ ނިއު އިންގްލެންޑް ޖާނަލް އޮފް މެޑިސިން ގައި “އަ ނޮވެލް ކޮރޯނާވައިރަސް ފްރޮމް ޕެއިޝެންޓްސް ވިތް ނިއުމޯނިއާ އިން ޗައިނާ، 2019 (އައު ވައްތަރެއްގެ ކޮރޯނާ ވައިރަސް އެއް ނިއުމޯނިއާ ބަލި ޖެހިފައިވާ ބަލި މީހެއްގެ ކިބައި 2019 ވަނަ އަހަރު ހޯދުން)” [7] މި ނަމުގަ އެވެ.
ވައިރަސް ފުރިހަމައަށް އައިސޮލޭޓް ނުކުރޭ:
- ފުއްޕާމޭގެ ދިޔަތައް ނެގި އެވެ.
- ސެންޓްރިފިއުޖަށް ލައްވާ ސެންޓްރިފިއުޖް ކުރި އެވެ.
- އޭގެ އެތެރެއަށް ފުއްޕާމޭގެ ކެންސަރު ސެލް އެޅި އެވެ.
- އެއަށް ފަހު، އެ ސާފުކޮށް އިލެކްޓްރޯން މައިކްސްކޯޕުން ބެލި އެވެ.
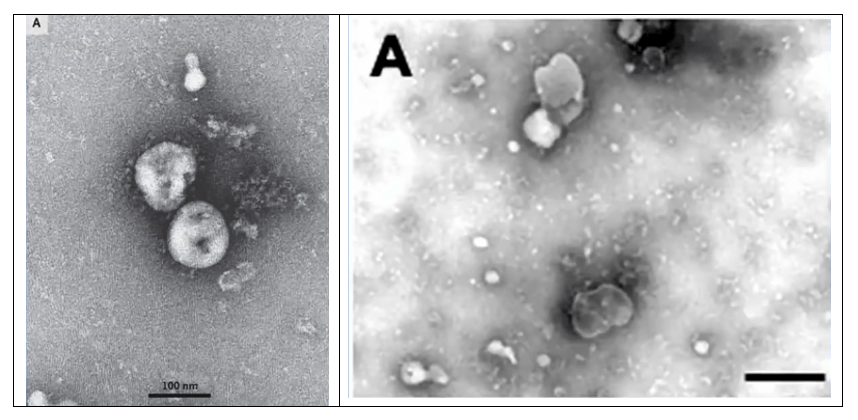
އައު-ކޮރޯނާ ވައިރަސް އެއް ކަމުގައި ބުނެފައިވަނީ ސީކުއެންސް އައިޑެންޓިޓީ %90 އަށް ވުރެ ދަށުން އެއްގޮތް ކަމުގައި ފެންނާތީ އެވެ.
Since the sequence identity in conserved replicase domains (ORF 1ab) is less than 90% between 2019-nCoV and other members of betacoronavirus, the 2019-nCoV — the likely causative agent of the viral pneumonia in Wuhan.
ކޯޗްސް ޕޯޗުލޭޓް ފުރިހަމަ ނުކުރޭ:
މި ދިރާސާގައި ބުނެފައިވަނީ “ޗައިނާ. ވޫހާންގެ ތިން ބަލި މީހުންނަށް ބޮޑުވަރު ވެފައިވާ ނިއުމޯނިޔާ ޖެހުނު ސަބަބު ކަމުގައި ގާތްކުރަނީ އައު ވައްތަރެއްގެ ބެޓާކޮރޯނާވައިރަސް އެއް” ކަމުގަ އެވެ.
“We describe in this report the use of molecular techniques and unbiased DNA sequencing to discover a novel betacoronavirus that is likely to have been the cause of severe pneumonia in three patients in Wuhan, China.” [8]
މި ދިރާސާގައި ބުނެފައިވަނީ “އަހަރެމެންގެ ދިރާސާ ކޯޗްސް ޕޯސްޗުލޭޓްސް ފުރިހަމަކޮށްފައި ނުވޭ، އެހެނަސް، ވޫހާން ގައި ބަލިމަޑުކަން ދިމާވުން 2019އިގެ އައު ކޮރޯނާ ވައިރަސް (2019-nCoV) ސަބަބައްވުން ދޭހާވާ ކަމުގައި އަހަރެމެންގެ އެނަލިސިސް ހެކި ފޯރުކޮށްދެ އެވެ.”
“Although our study does not fulfill Koch’s postulates, our analyses provide evidence implicating 2019-nCoV in the Wuhan outbreak.”
ފުރަތަމަ މިތަނުގައި ކޯޗްސް ޕޯޗުލޭޓްގެ ވާހަކަ ގެނައުމުން އެނގިގެން ދަނީ ވައިރަސް އަކުން ބަލި ޖައްސާ ކަން ސާބިތުކުރުމަށް ކޯޗްސް ޕޯޗުލޭޓް މުހިންމު ވެގެންވާ ކަމެވެ. ކޯޗްސް ޕޯޗުލޭޓް މުހިންމު ނޫން ނަމަ އެމީހުން އޭގެ ވާހަކަ ޒިކުރު ކުރުމުގެ މާނަ އެއް ނެތެވެ. ދެވަނައަށް ޗައިނާގެ ވޫހާންގައި ބަލިމަޑުކަމެއް ފެރުރިގެން އުޅެނީ އައު ކޮރޯނާ ވައިރަސް އަކުން ކަމުގައި “ހެކިތައް އިންޕްލިކޭޓް” ކުރާކަމަށް ނުވަތަ ދޭހަވާ ކަމުގައި އެވަނީ ވިދާޅުވެފަ އެވެ. އޭގެ މާނައަކީ އެމީހުންނަށް ޔަޤީނުގެ ދަރަޖަ ނެތް ކަމެވެ. އަދި އެއީ އެމީހުންގެ ޚިޔާލީ ނަޒަރެއް ނުވަތަ ހައިޕޮތެސިސް އެއް ކަމެވެ.
1937 ރިވާސް ބުނެފައިވެ އެވެ. “ވައިރަލް ބަލިތަކުގައި ކޯޗްސް ޕޯޗުލޭޓް ފުރިހަމަވެފައި ނުވާކަން ފާޅުކަންބޮޑުކޮށް އެނގެ އެވެ.”
“It is obvious that Koch’s postulates have not been satisfied in viral diseases.”[9]
ސާރސް-ކޮވް-2 ގެ ފުރިހަމަ ޖީނޯމް ސީކުއެންސް ހުރި ކަމުގައި ނެރެފައިވާ ޕޭޕަރު ތަކުގައިވާ (ކޮމްޕްލީޓް ޖީނޯމް) ސީކުއެންސަކީ ކޮންޕިއުޓަރ ސޮފްޓްވެއާރ އަކުން ފަރުމާކޮށްފައިވާ ޚިޔާލީ ޖޯނޯމް އެކެވެ.
ޕޯސްޗުލޭޓް 1: ހުރިހާ ކޭސް އެއްގައި ވައިރަސް ފެންނަންވާނެ.
- ބަލި މީހާގެ ކިބައިން ނެގި އެއްޗަށް އިތުރު އެއްޗެއް މަސްހުނި ނުކޮށް ސީދާ ވައިރަސް “ޕާޓިކަލް” އެއް ހޯދަފަ އެއް ނެތް
- (2) އެމީހުން ވައިރަސް އޭ ކިޔާފައި ހޯދި އާރްއެންއޭ މާއްދާގެ އަޞްލަކީ ކޮބާ ކަން ހަޤީޤަތުގައި ނޭނގޭ، ސަބަބަކީ އެޔަށް އެހެން އެއްޗެހި އެއްކުރި، އެއްކުރި އެއްޗަކުން ނުކުތް، އާރްއެންއޭ އެއް ކަމަށް ވެދާނެ، އަދި އާރްއެންއޭ އަކީ ކުރު ސީކުއެންސްކޮޅެއް. އަދި ކެމިކަލީ ވައިރަލް އާރްއެންއޭ އެއް ކެރެކްޓަރައިޒްކޮށް (ސިފަކޮށް) އަދި ސާފުކޮށްފައިވެސް ނުވޭ.
- (3) މައިކްސްރޯޕުގެ ޒަރީޢާއިން ދައްކާފައިވާ ޕޮޓޯތަކަކީ ސެލް ކަލްޗާ (ސެލްއަށް އޭތި މީތި އެޅުމައްފަހު ހަދާފައިވާ ސޫޕު ގަނޑަކުން) ނަގާފައިވާ ފޮޓޯތަކެއް، އެއީ ކޮން އެއްޗެއްގެ ފޮޓޮއެއް ކަމެއް ނޭނގޭ.
- (4) ހަމައެކަނި 3 މީހުންގެ މައްޗަށް ހަދާފައިވާ ތަހުލީލެއް. އެހެންކަމުން ބާކީތިބި 200 މީހުންނަށް ބަލި ޖެހުނީ އޭނގެން ކަމުގެ ހެއްކެއް ނުނިންމޭނެ.
ޕޯސްޗުލޭޓް 2: ސާފުކުރެވިފައިވާ ވައިރަސް (ޕިއުރިފައިޑް ވައިރަސް)
- ޒަހޫ ޕޭޕަރުގައި ސެކް ކަލްޗާއިން ހޯދާފައިވާ މެޓީރިއަލް (ބަޔަކީ) ސާފު (ޕިއުރ) ވައިރަލް ޕާޓިކަލްސްތަކެއް ނޫން އަދި އޭގައި މަކުނުގެ ސެލް (Vero E6)، ދިރުވާ މީޑިއަމް (DMEM)، ފެޓަލް ބޮވައިން ސިރަމް ()، ޕެނިސިލިން (penicillin) އަދި ސްޓްރެޕްޓޯމައިސިން (streptomycin) ހުއްޓެވެ. ވައިރަސް އޭ ކިޔައިގެން އެމީހުން ހޯދައިގެން އުޅޭ އެއްޗެއް ހޯދުމަށް އެމީހުން ކުރި ކަމަކީ 3 ބަލި މީހުންގެ ފުއްޕާމޭގެ ދިޔަ ނަގައި، އެޔަށް މަކުނުގެ ކިޑްނީ ސެލް އަޅައި، އޭތެ ކަލްޗާއެއްގައި ދިރުވި (ގްރޯކުރި) އޭގައިވާ ސެލްތައް މަރުވަންދެން، އެދި އެޔަށް ބޮވައިން ކައުފް ސިރަލް އެޅި އެވެ. ބޮވައިން ކައުފް ސިރަމް އަކީ ކުޑަ ކައު (ބަކަރީގެ) ލޭގެ ބައެކެވެ. އަދި އެޔަށް އަނެއްކާ އެމީހުންވަނީ އެންޓިބަޔޮޓިކްތައް (ޕެނެސިލިން އަދި ސްޓްރެޕްޓޯމައިސިން) އަޅާފަ އެވެ. އެންޓި ބަޔޮޓިކް އަކީ ސެލްއަށް ހުށަހެޅުމުން ސެލްއިން އެކްސެޒޯމްސް ބޭރުކުރާ އެއްޗެކެވެ.
- ޤުދުރަތީ ގޮތުން ބަލި ހުރި މީހެއްގެ ކިބައިން ނެގިފައިވާ އެއްޗެއް ނޫން އެއީ، އެ އެއްޗެއް ނަގާފައިވަނީ ސެލް ކަލްޗާތަކުގައި އަމިއްލައަށް ލެބޯރޓަރީގައި އުފައްދާފައިވާ އެއްޗަކުން ނެވެ.
5 މެއި 2020 ގެ ޕޭޕަރު: ވައިރަސް ހޯދާފައިވާ ކަމަށް ނެރެފައިވާ އަނެއް ދިރާސާ ނެރެފައިވަނީ ޗައިނީސް މެޑިކަލް ޖާނަލް ގައި “އައިޑެންޓިފިކޭޝަން އޮފް ނޮވެލް ކޮރޯނާވައިރަސް ކައުސިން ސިވިއާ ނިއުމޯނިއާ އިން ހިއުމަން: އަ ޑިސްކްރިޕްޓިވް ސްޓަޑީ” ނަމުގަ އެވެ. [10]
ކޯޗްސް ޕޯޗުލޭޓް ފުރިހަމަ ނުކުރޭ:
މި ދިރާސާގައި ބުނެފައިވަނީ “ބަލި މީހުންގެ ކިބައިގައި އުފެދުނު ނިއުމޯނިއާއާއި އައު ކޮރޯނާ ވައިރަސް ގެ ގުޅުމެއް (އެސޯސިއޭޝަން) އެއް ވާކަން މި ހޯދުންތައް އިންޑިކޭޓް (ދޭހަކޮށްދެ) އެވެ.”
These findings primarily indicate that the novel CoV is associated with the pneumonia that developed in these patients. However, it remains to be determined whether this novel CoV is capable of causing similar diseases in experimental animals.
In conclusion, we identified a novel bat-borne CoV associated with a severe and fatal respiratory disease in humans.
އެސޯސިއޭޝަން އަކީ އަދި ކައުޝުއަލިޓީ އެއް ނޫނެވެ. މި ޕޭޕަރު ވެސް ކޯޗްސް ޕޯޗުލެޓެއް ފުރިހަމަ ކޮށްފައި ނުވެ އެވެ.
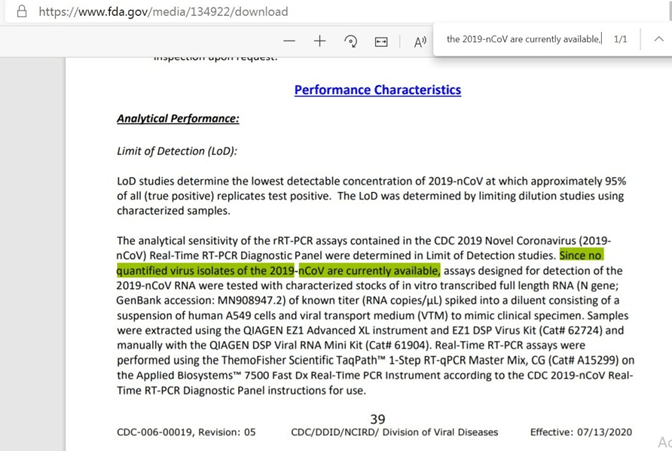
13 ޖުލައި 2020: ޚުދު އެމެރިކާގެ ސީޑީސީ އާއި އެފްޑީއޭއިންވެސް ވަނީ ކޮވިޑް-19 ވައިރަސް އައިސޮލޭޓް (ހޯދައި ވަކި) ކުރެވިފައި ނުވާ ކަމުގައި 13 ޖުލައި 2020 ގައި އެމީހުން ނެރުނު ކޮވިޑް-19 އިރުޝާދު ކަރުދާހުގައި ލިޔެފަ އެވެ. “
ޕީސީއާރް ޓެސްޓު ޕޭޕަރުގެ އުނި އެތައް ކަމެއް:
ކޯރމަން- ޑްރޮސްޓެން ހިޔަޅު ޕިސީއާރް ޕޭޕަރު

21 ފެބުރުއަރީ 2020: “ޑިޓެކްޝަން އޮފް 2019 ނޮވެލް ކޮރޯނާ ވައިރަސް (2019-nCoV) ބައި ރިއަލް-ޓައިމް ޕީސީއާރް” [11] ކިޔައި ފަންނީ ޕޭޕަރެއް ފެބުރުއަރީ 21 ގައި ޔޫރޯސަވެއިލްނެސް ޖާނަލް އަށް ހުށައެޅުނެވެ. މި ޕޭޕަރުގެ އެންމެ އިސް މުއްލިފުންނަކީ ޖަރުމަންގެ “ވައިރޮލޮޖިސްޓު” ކްރިސްޓިއަން ޑްރޮސްޓެން (Christian Drosten) އަދި ވިކްޓޯ ކޯރމަން އެވެ. ކްރިސްޓިއަން ޑްރޮސްޓެން އަކީ 2003 ވަނަ އަހަރު ސާރްސް (SARS) ކޮރޯނާ “ވައިރަސް” ކޯ-ޑިސްކަވަރ ކޮށް އެޔަށްވެސް ޓެސްޓު އުފެއްދި މީހާ އެވެ. މީނާ އަކީ ޖަރުމަންގެ ބާރލިންގެ ޗަރައިޓް އިންސްޓިޓިއުޓް އޮފް ވައިރޮލޮޖީގެ އެންމެ އިސް މީހާ އެވެ.
ޔޫރޯސަވެއިލްނެސް ޖާނަލް
23 ފެބުރުއަރީ 2020: “ޑިޓެކްޝަން އޮފް 2019 ނޮވެލް ކޮރޯނާ ވައިރަސް (2019-nCoV) ބައި ރިއަލް-ޓައިމް ޕީސީއާރް” ކިޔާ ޕޭޕަރު ޔޫރޯސަވެއިލްނެސް ޖާނަލް އަށް ހުށައެޅިތާ 24 ގަނޑި އިރުތެރޭ މި ޕޭޕަރު ޕިއަރ ރިވިއު ކުރުމެއް ވެސް ނެތި ވަނީ މި ޖާނަލްގައި ޝާއިއުކޮށްފަ އެވެ. ޔޫރޯސަވެއިލެންސް ޖާނަލް ގައި އެންމެ އަވަހަށް ލިޔުމެއް ޝާއިއުކޮށްފައި ވަނީ 124 ދުވަސް ތެރޭގަ އެވެ. މިހެން މިކަން އޮތް އިރު ޕިއާ-ރިވު ކުރުމެއް ވެސް ނެތި އަވަސް އަރުވާލައިގެން މި ޕޭޕަރު ވަނީ މި ޖާނަލްގައި ޝާއިޢުކޮށްފަ އެވެ. މިއީ އެ ޕޭޕަރަކަށް ބިނާކޮށް ޑަބްލިޔުއެޗްއޯ އިން މުޅި ދުނިޔޭގައި ކޮވިޑް-19 ބަލި ޖެހިފައި ހުރިތޯ ބެލުމަށް މުޅިދުނިޔޭގައި ފަށާފައިވަނީ މި ދިރާސާ ޕޭޕަރެވެ. މި ޕޭޕަރާއި އެކު ޑަބްލިޔުއެޗްއޯއިން އެމީހުންގެ ދަށުގައިވާ މުޅި ދުނިޔޭގެ އެންމެހައި ޞިއްޙީ އެޖެންސީތަކަށް މި ޕޭޕަރުގައި އަންގާފައިވާ ގޮތަށް ޕީސީއާރު ޓެސްޓުކޮށް ކޮވިޑް -19 އަށް ޑައިގްނޮސްޓިކް ޓެސްޓުތައް ކުރިއަށް ގެންދިޔުމަށެވެ.
We aimed to develop and deploy robust diagnostic methodology for use in public health laboratory settings without having virus material available.
މާނައަކީ: ވައިރަސް އަހަރެމެން އަތުގައި ނެތް ހާލު އަހަރެމެން ބޭނުންވަނީ ކޮވިޑް-19 ވައިރަސް ހޯދުމަށް ޓެސްޓެއް އުފެއްދުމަށެވެ.
މި ޕޭޕަރުގެ އެންމެ ކޯޅުމާއި މައްސަލަ ބޮޑު ކަމެއް ކަމުގައި ފާހަނގަ ކުރެވިފައިވަނީ ސާރސް-ކޮވް-2 (SARS-CoV-2 ) ކިޔާ ވައިރަސް އަށް އެމީހުން މި ޓެސްޓު ހަދަން ފަރުމާކޮށްފައި ވަނީ އެމީހުންގެ އަމިއްލަ އިއުތިރާފާއި އެއްބަސް ވުމުން އަސްލު އެކިޔާ “ވައިރަސް މެޓީރިއަލް ލިބެން ނެތް ހާލުގައި” ޗައިނާގެ ސައިންސުވެރިން އިންޓަނެޓްގައި ޝާއިއުކޮށްފައިވާ ޖެނެޓިކް ސީކުއެންސު ތަކަކަށެވެ. އަދި މި ޓެސްޓު ވެލިޑޭޓް ކޮށްފައިވަނީ 2003 ވަނަ އަހަރު އެމީހުން ހޯދައިގެން އެޅުނު ކަމުގައި ދަޢުވާކުރި ސާރސް-ކޮވް1 އާއި އޮތް ޖެނެޓިކް ގުޅުމުގެ މައްޗަށް ބިނާކޮށް ސިންތެޓިކް ނިއުކްލިއެކް އެސިޓް ޓެކްނޮލޮޖީގެ ޒަރީޢާއިން ނެވެ. ތިރީގައިވަނީ އެ ޕޭޕަރުގައި ސީދާ ލިޔެފައިވާ އިބާރާތެވެ.
“Designed in absence of available virus isolates or original patient specimens.. Design and validation were enabled by the close genetic relatedness to the 2003 SARS-CoV, and aided by the use of synthetic nucleic acid technology.”[12]
އެހެނަސް، ހިތާމަ އަކީ މި ވާހާކަ ތިޔަ ބޭފުޅުންގެ މިނިވަން މުސްތަޤިލު މީޑިއާތައް ކަމަށް ދަޢުވާ ކުރާ އެއްވެސް މީޑިއާއަކުން ގެނެސްދީފައި ނުވެ އެވެ.
ފުރަބަންދު (ލޮކްޑައުން) އަދި އިޤްތިޞޯދު ފުނޑާލުން:
މި ޓެސްޓު ޕޭޕަރާއެކު އައި މަސްތަކުގައި ޤައުމުތައް ފުރަބަންދުކޮށް، ޤައުމުތަކުގެ އިޤްތިޞޯދުތައް އަދަވަޅަކަށްވައްޓައި، ސްކޫލްތައް ބަންދުކޮށް ކުޑަކުދިން ކިޔެވުމުގެ ހައްޤުން މަޙުރޫމްކޮށް، ބިރުވެރިކަމާއި ޕެނިކް އުފައްދައި އެކިއެކި ހަރަކާތްތައް ކުރިޔަށް ގެންދަށް ފެއްޓުނެވެ.
27 ނޮވެންބަރ 2020: ކޮރްމަން-އަދި-ޑްރޮސްޓޮން ޕޭޕަރު “ޑިޓެކްޝަން އޮފް 2019 ނޮވެލް ކޮރޯނާ ވައިރަސް (2019-nCoV) ބައި ރިއަލް-ޓައިމް ޕީސީއާރް” އަށް ޗެލެންޖުކޮށް 22 ބައިނަލް އަޤްވާމީ ސައިންސުވެރިއެއް ވަނީ މި ޕޭޕަރުގައިވާ 10 ބޮޑު މައްސަލައެއް ފާހަގަކޮށް މި ޕޭޕަރު ބާޠިލް ކުރުމަށް އެދި ޔޫރޯސަވެއިލްނެސް ޖާނަލް އަށް ޕިއާ-ރިވިއު ޕޭޕަރެއް ހުށައަޅާފަ އެވެ. އެ ޕޭޕަރުގެ ނަމަކަށް ދެވިފައިވަނީ “އެކްސްޓާރނަލް ޕިއާ ރިވިއު އޮފް އާރްޓީޕީސީއާރް ޓެސްޓު ޓު ޑިޓެކްޓް ސާރސް-ކޮވް-2 ރިވީލް 10 މޭޖާ ފްލޯސް އެޓް ދި މޮލެކިއުލާ އެންޑް މެތޮޑޮލޮޖިކަލް ލެވެލް” މިފަދައިނެ އެވެ. އެބަހީ، ސާރސް-ކޮވް-2 ވައިރަސް ހޯދުމަށް ހަދާ އާރްޓީ-ޕީސީއާރް ޓެސްޓުގެ (ކޮރްމަން-ޑްރޮސްޓޮން ޕޭޕަރު) ގެ މައްޗަށް ފަންނީ ގޮތުން އިސް ބަޔަކު ޖާނަލްއިން ބޭރުން ހަދާފައިވާ މުރާޖަޢާ ކުރުމުން ދައްކަނީ މޮލެކިއުލާ އަދި މަންހަޖީ ލެވެލް އެއްގައި 10 ބޮޑު އުނިކަން ވާކަން” މި އެވެ.
މި ޕޭޕަރުގެ އެންމެ އިސް މުއައްލިފަކީ ޑރ. ޕީޓާރ ބޮރގާ (Dr. Pieter Borger) އެވެ. މި ބޭފުޅާ އަކީ މޮލެކިއުލާ ބަޔޮލޮޖީ އޮފް ޖީން އެކްސްޕްރެޝަން ގައި ފަންނީ މާހިރެކެވެ. މީގެ އެހެން ފާހަގަކޮށްލެވޭ މުއައްލިފުންގެ ތެރޭފައި ވެކްސިން އުފައްދާ ފައިޒާ ކުންފުނީގެ ކުރީގެ ވީޕީ ޑރ. މީކާއީލް ޔީޑޮން (Dr. Michael Yeadon) ހިމެނެ އެވެ.
ޓެސްޓުކުރެވޭ އެތީގެ އަޞްލު ނެތި ޓެސްޓު ފަރުމާކޮށް ޓެސްޓު ކުރެވެން ފެއްޓުން:
އެމިރިކާގެ ޖާނަލިސްޓް ސެލިއާ ފާބާ މި ރިވިއު ޕޭޕަރު ލިޔުއްވި އެއް ސައިންސުވެރިޔެއް ކަމުގައިވާ ޑރ. ކެވިން ކޯރބެޓް (Dr. Kevin Corbett) އާއި ސުވާލުކުރުމުން ޑރ. ޑރ. ކެވިން ކޯރބެޓް ވިދާޅުވެފައިވަނީ މިފަދައިން ނެވެ. “މި ޕޭޕަރުން ވަނީ (ކޮވިޑަށް ޕީސީއާރް) ޓެސްޓު ކުރުމަށް އުފައްދާފައިވާ އެންމެހައި ސައިންސުގެ ބުއްދީގެ ހަމަތައް ހަލާކުކޮށް ނެތިކޮށްލާފަ އެވެ. ޑްރޮސްޓޮން (ކޮވިޑަށް ޕީސީއާރް) ޓެސްޓު އުފެއްދި އިރު، ޗައިނާއިން އެމީހުންނަށް ވައިރަލް އައިސޮލޭޓެއް ދީފައި ނުވެ އެވެ. އެމީހުން ޓެސްޓު ތައްޔާރުކުރީ ޖީން ބެންކުގައިވާ ސީކުއެންސަކުން ނެވެ. ތިބާއަށް ފެނޭ ހެއްޔެވެ؟ ޗައިނާއިން އެމީހުންނަށް ޖެނެޓިކް ސީކުއެންސް ދިނީ އެއާއި ގުޅޭ ވައިރަސް އައިސޮލޭޓް އާއި ނުލަ އެވެ. އެމީހުން އަތުގައި ކޯޑެއް އޮތް އެހެނަސް އެކޯޑާއި ބެހޭ އެއްވެސް އެއްޗެއް ނެތެވެ. އެއްވެސް ވައިރަސް މޮރފޮލޮޖީ އެއް ނެތެވެ.” [13] ޑޮކްޓަރު ކުރެން ސެއިލާ ވައިރަސް މޮރފޮލޮޖީ އަކީ ކޮބައިތޯ އާންމު މީހަކަށް ހަކަށް ތައުރީފްކޮށްދޭށޭ ވިދާޅުވުމުން ޑރ. ކެވިން ކޯރބެޓް ވިދާޅުވެފައިވަނީ މިސާލަކަށް “މަސް މާރުކޭޓެއްގައި މީހަކަށް ކަށިތަކެއް ދިނުމަށްފަހު އެއޮތީ ކަލޭގެ މަހޭ ބުނުންފަދަ ކަމެކެވެ. އެއީ ކޮންމެ މަކެއް ކަމައް ވެސް ވެދާނެ އެވެ. އޭނަ ދިނަނީ މުޅި ކަށިފައްޗެއް ވެސް ނޫވެ. މިއޮތީ ކަށިތަކުގެ ކުޑަ ކުޑަ އެތިކޮޅެކެވެ. އެއީ ކަލޭގެ މަހެވެ. އަޑުއަހާށެވެ. ކޮރމަން/ޑްރޮސްޓެން ގެ ޕޭޕަރުގައި ބަލި މީހެއްގެ ފަރާތުން ނެތި އެއްވެސް އެއްޗެއް ނެތެވެ. އެހުރިހާ އެއްޗެއް ހުރީ ޖީން ބެންކުން ނެގިފަ އެވެ. އަދި ވައިރަސްގެ ސީކުއެންސުގެ އެތިތިކޮޅުތައް އޭގައި ނެތް އެއްޗެހިން އެމީހުން އެ އުފެއްދީ އެވެ. އޭތި އެމީހުން ހެދީ ސިންތެޓިކަލީ (އިންސާނުން އަމިއްލަޔަށް) (ޖީންގެ) ހުސްތަންތަން އެމީހުން ފުރާލުމަށެވެ. ޖެނެޓިކްސް އަކީ އެއީ އެވެ. އެއީ ކޯޑެކެވެ. އެއީ އެހެންކަމުން އޭބީބީބީސީސީޑީޑީޑީ އަދި ކަލޭ އީއީއީ ކަމުގައި ހީކުރާ އެއްޗެއް އޭގައި މަދުވުވުން ކަލޭ އެއަށް އެ އެއްކުރަނީ އެވެ. އެއީ މުޅިންވެސް އަމިއްލައަތުން ހަދާފައިވާ (ސިންތެޓިކް) އެއްޗެކެވެ. މަދުވާ އެތިކޮޅުތައް ތިބާ ހަމަ އުފައްދަނީ އެވެ. މީއީ ވައިރޮލޮޖީ ޖެނެޓިޒަޒޭޝަން ކުރުމުގެ ނަތީޖާ އެވެ. މައިގަނޑު ގޮތެއްގައި މިއީ ކޮންޕިއުޓަރ ވައިރަސް އެކެވެ.”
“Every scientific rationale for the development of that test has been totally destroyed by this paper. It’s like Hiroshima/Nagasaki to the Covid test,” “When Drosten developed the test, China hadn’t given them a viral isolate. They developed the test from a sequence in a gene bank. Do you see? China gave them a genetic sequence with no corresponding viral isolate. They had a code, but no body for the code. No viral morphology.” I asked him to define “viral morphology” for the layperson. “In the fish market,” he said, “it’s like giving you a few bones and saying that’s your fish. It could be any fish. Not even a skeleton. Here’s a few fragments of bones. That’s your fish. Listen, the Corman/Drosten paper, there’s nothing from a patient in it. It’s all from gene banks. and the bits of the virus sequence that weren’t there they made up. They synthetically created them to fill in the blanks. That’s what genetics is; it’s a code. So its ABBBCCDDD and you’re missing some what you think is EEE so you put it in. It’s all synthetic. You just manufacture the bits that are missing. This is the end result of the geneticization of virology. This is basically a computer virus.
ކޮރްމަން-ޑްރޮސްޓޮން ޕޭޕަރު ޖާނާއިން ބޭރުކޮށް އެޕާޕަރު ރިޓްރެކްޓް (ބާޠިލު ކުރުމަށް) ހުށައަޅާފައިވާ 22 ސައިންސުވެރިންގެ ތެރެއިން އެކަކީ ޑރ. ޕީޓާ ބޯޖާ، ޕީއެޗްޑީ (Dr. Pieter Borger) އެވެ. ޑރ. ޕީޓާ ބޯޖާ އަކީ މޮލެކިއުލާ ޖެނެޓިކްސް ގެ އެކްޕާޓެއް ނުވަތަ ފަންނީ މާހިރެކެވެ.މި ބޭފުޅާގެ 70 އަށްވުރެ ގިނަ އެކިއެކި ބޭޕަރުތައް މަޝްހޫރު މެޑިކަލް ޖާނަލްތަކުގައި ނެރެފައިވެ އެވެ. [14] ޕީސީއާރް ޓެސްޓާއި މެދު މި ބޭފުޅާ ވިދާޅުވެފައިވަނީ “(ޕީސީއާރް ޓެސްޓުން) ހޯދަނީ (ޑިޓެކްޓުކުރަނީ) ވައިރަސް އެއް ނޫނެވެ.”
“You are not detecting a virus.”
“Once I heard a good comparison. If you go to a junkyard and you find a wheel or a hubcap from a Mercedes, and a steering wheel of a Mercedes, can you infer that you are in a Mercedes garage at that moment? If you only see those two parts? No, you can’t. You don’t know anything about it… you only know you have a steering wheel, you can find those things everywhere. In every junkyard you can find them.” “no relevance for the diagnosis whatsoever.”
ޑރ. ޕީޓާ ބޯޖާ ވިދާޅުވިއެވެ. “އަހަރެން ޕީސީއާރް ޓެސްޓާއި މެދު ރަނގަޅު އަޅާކިޔުމެއް އަޑުހީމެވެ. ޖަންކްޔާޑަށް (ނުވަތަ ހަލާކުވެފަ ހުންނަ ކާރު އުކާލާފަ ހުންނަ ތަނަކަށް) ގޮސް މާރސިޑީސް ކާރެއްގެ ފުރޮޅަކާއި އޭގެ ހަބްކެޕާއި އަދި އޭގެ ސްޓިއަރިން ވީލް ނެގީ އެވެ. އެތަނުން އެ ނެގުމުން ތިބާ އެކުރީ މާރސިޑީސް ގަރޭޖެއްގައި ކަމުގައި ބުނެވެނޭ ހެއްޔެވެ؟ ތިބާއަށް ހަމައެކަނި އެ ދޭތި ފެނުމުން؟ ނޫނެކެވެ. ނުބުނެވޭނެ އެވެ. ކަލެއަށް އެނގޭ ކަމަކީ ކަލޭ އަތުގައި ސްޓްއަރިންވީލް އޮތް ކަމެއް. އެއީ ކޮންމެ ތާކުން ވެސް ފެނިދާނެ އެއްޗެކެވެ. ކޮންމެ ޖަންކު ޔާޑަކުން ވެސް އެ ފެނިދާނެ އެވެ. އެއީ ބައްޔަކަށް ޑައިގްނޯސް ކުރުމަށް އެއްވެސް ގުޅުމެއް އޮތް އެއްޗެއް ނޫނެވެ.”
ޕީސީއާރް ޓެސްޓުން ވައިރަސް އާރް އެންއޭ ދެއްކުމަކީ މީހާ ބަލި މީހެއްކަމުގައިވުން ނޫން، އެފަދައިން ބުނަނީ ސިއްހީ ފްރޯޑުން
އެމެރިކާގެ ސީޑީސީން ނެރެފައިވާ ޕޭޕަރުގައި ލިޔެފައިމިވަނީ ޕީސީއާރް ޓެސްޓުން “ވައިރަލް RNA އާރް.އެން.އޭ ހުރިކަމަށް ދެއްކުމަކީ އިންފެކްޝަސް ވައިރަސް އެއް ހުރިކަމަށް ނުވަތަ ކޮވިޑް19 އަކީ އެމީހެއްގެ ބަލީގެ އަލާމާތްތައް (ރޯގާ، ހުން އައުން، ކެއްސުން، ނިއުމޯނިއާ) މެދުވެރިކުރި އެޖެންޓު (މާއްދާ) ކަމުގައި ނުވެ ހިނގައިދާނެ އެވެ.”
“Detection of viral RNA may not indicate the presence of infectious virus or that 2019-nCoV is the causative agent for clinical symptoms.”[15]
މާނައަކީ: ކޮވިޑް19 އަށް ފައްސިވުމަކުން އަދި އެމީހާ ގެ ބަލީގެ އަލާމާތްތައް ފެނިގެން އުޅެނީ ކޮވިޑް19 ގެ ސަބަބުން ކަމަށް އެއިން ދަލީލުކޮށްނުދެ އެވެ. އެހެންކަމުން އެމީހާ އަކީ ބަލި މީހެއްކަން މި ޓެސްޓުން ޔަޤީން ނުކޮށްދޭ އިރު މިއަށް އިތުބާރުކޮށް ޕޮޒިޓިވް ވާއިރަށް ބަލި މީހެއް ކަމުގައި ނިންމަނީ ކީއްވެތޯ އެވެ.
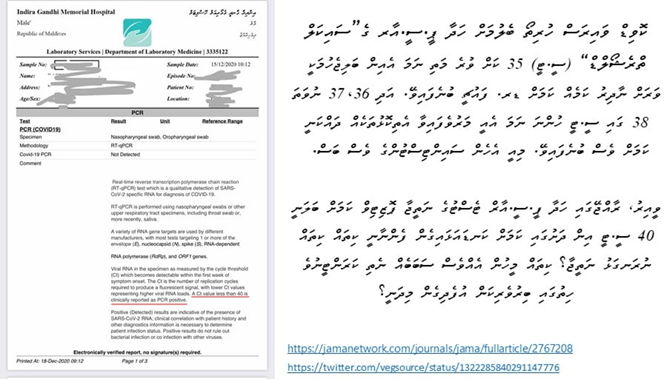
ސައިކަލް ތެރެޝޯލްޑް:
ކޮވިޑް ވައިރަސް ހުރިތޯ ބެލުމަށް ހަދާ ޕީ.ސީ.އާރ ގެ “ސައިކަލް ތްރެޝޯލްޑް” (ސީ.ޓީ) 35 ކަށް ވުރެ މަތި ނަމަ އެއިން ބަލި ޖެހުމަކީ ވަރަށް ނާދިރު ކަމެއް ކަމައް އެމެރިކާގެ ޑރ. ފައުޗީ ބުނެފައިވެ އެވެ. އަދި 36. 37 ނުވަތަ 38 ގައި ސީ.ޓީ ހުންނަ ނަމަ އެއީ މަރުވެފައިވާ އެތިކޮޅުޅަކެއް ދައްކަނީ ކަމަށްވެސް އޭނާ ބުނެފައިވެ އެވެ.
8 ޖޫން 2020: ފައުޗީ ބުނެފައިވެ އެވެ. “އެ ބިނާވެގެންވަނީ ސައިކަލް ތްރެޝޯލްގެ މައްޗަށް ކަމުގައި އަހަރެމެންނަށް ހީވާން ފައްޓައިފި އެވެ. އޭގެ މާނައަކީ ޕޮޒިޓިވް އާއި ހިސާބަށް ވާޞިލްވުމަށް ޕީސީއާރް ސައިކަލް ކުރިއަށް ގެންދަނީ ކިހާ ގިނަ އަދަދަކަށް ތޯ އެވެ. 35 އަދި އެއަށް ވުރެ އިތުރު (ސައިކަލް އަށް ހަދާފަ) ޓެކްނިކަލީ ޕޮޒުޓިވް ވިޔަސް، އިންފެކްޝިއަސް ވުމުގެ ބާރު ވަރަށް ވެސް ބޮޑަށް ދަށްވެގެން ވެއެ އެވެ. އެހެން ބަހަކުން ބުނާނަމަ، ޕީސީއާރް ޕޮޒިޓިވް ޓެސްޓެއް ތިބާއަށް އޮވެދާނެ އަދި އެޔާއެކު ތިބާ އަކީ ބަލިފަތުރާ މީހެއް ކަމުގައި ނުވެދާނެ އެވެ.”
Dr Fauci: “We’re starting to get a feel that it depends on the cycle threshold, which means how many times it takes you to do the PCR cycle to get a positive hit. If it’s 35 or more, even though it’s technically positive, the chances of that being replication competent are extremely low. In other words, you could have a PCR-positive test and yet still not be contagious.”[16]
16 ޖުލައި 2020: ފައުޗީ ބުނެފައިވެ އެވެ. “35 ސީޓީ މަތިން ނަގައިފިނަމަ، އޭތީގެ (އެކިޔާ ވައިރަހުގެ) އިތުރުވުމުގެ ބާރު (އިންފެކްޝިއަށްކަން) ވަރަށް ވެސް ކުޑަ އެވެ. 37 ތްރެޑްޝޯލްޓަކުން ކަލެޔަށް ވައިރަސް ކަލްޓިވޭޓް ކުރުމަކީ ނުވާނެ ކަމެކެވެ. މީހަކު 37، 38 އަދި 36 (ސައިކަލް) އިން (ޕޮޒިޓިވްގެން) އަޔަސް، ބުނަން ޖެހޭނީ އެއީ ހަމަ މަރުވެފައިވާ ނިއުކްލިއޯޑައިޑް (އާރްއެންއޭ ނުވަތަ ޑީއެންއޭ) އެކެވެ. މިހިސާބުން ނިންމާލާށެވެ.”
Dr. Fauci: “If you get a Ct of >=35, the chances of it being replication competent (i.e., infectious) are miniscule. You almost never can culture virus from a 37 threshold cycle. If somebody does come in with 37,38, even 36, you gotta say it’s just dead nucleotides. Period.”[17]
28 ސެޕްޓެންބަރ 2020:
At Ct = 35, the value we used to report a positive result for PCR, <3% of cultures are positive.[18] the accuracy dropped to 3%, meaning up to 97% of positive results could be false positives.
ކޮވިޑް-19 އިންފެކްޝަން ފެޓަލިޓީ ރޭޓް އޮޅުވާލުން:ް
ކޮވިޑް-19 ގެ ނުރައްކާ އިންފްލުއެންޒާ އާއި އެއްވަރެއް ކަމުގައި އޮކްޓޯބަރު 2020 ގައި ޑަބްލިޔުއެޗްއޯއިން ވަނީ އިޤުރާރުވެ އެމީހުންގެ ވެބްސައިޓްގައި ޑރ. ޖޯން އައޮނިޑިސް (ސްޓޭންފޯޑް ޔުނިވާސިޓީގެ ޕްރޮފެސަރ އޮފް މެޑިސިން އަދި ޕްރޮފެސަރ އޮފް އެޕިޑިމިއޯލޮޖީ އެންޑް ޕޮޕިއުލޭޝަން ހެލްތު) ގެ ފަންނީ ހޯދުން ޝާޢިއުކޮށްފަ އެވެ.[19]
In people < 70 years, infection fatality rates ranged from 0.00% to 0.31%
އެސިމްޓޮމެޓިކް އިންފެކްޝަން އަކީ ނެތް އެއްޗެއް:
ފާމައުއިޓިކްލް އިންޑަސްޓްރީއާއި ދެކޮޅަށް ވިސެލްބްލޯ ކުރި އަދި ޕީސީއާރް ކޭސްޑެމިކްއާއި ދެކޮޅަށް ތެދުވެފައިވާ ޖަރުމަންގެ މަޝްހޫރު ލޯޔަރު، ރެއިނާރ ފުއެލްމިޗް (Reiner Fuellmich) ވިދާޅުވެފައިވަނި “އަހަރެން ޤަބޫލުކުރާ ގޮތުގައި މި ކާޑުން ހަދާފައިވާ ގެ (ޕެންޑަމިކް) ވައްޓާލުމަށްޓަކައި އަހަރެމެން ހަމަލާދޭންވީ ޕީސީއާރް ޓެސްޓަށެވެ. ހަޤީޤަތަކީ ޢަލާމާތްތައް ނުފެންނަ އިންފެކްޝަން (އެސިމްޕްޓޮމެޓިކް އިންފެކްޝަން) އަކީ އެއީ ނެތް އެއްޗެކެވެ.”
German lawyer who is central to a growing group of lawyers, scientists, politicians, and even secret pharmaceutical whistleblowers, said in an interview, “We believe that in order to make this house of cards collapse, we have to attack the PCR test. The fact is, there are no asymptomatic infections.”
20 ނޮވެންބަރ 2020: “ޕޯސްޓް-ލޮކްޑައުން ސާރސްކޮށް2 ނިއުކްލިއެކް އެސިޑް ސްކްރީނިން އިން ނިއާލީ ޓެން މިލިއަން ރެސިޑެންޓްސް އޮފް ވޫހާން، ޗައިނާ” މި ނަމުގައި ނެރެފައިވާ ދިރާސާއިން ވަނީ އެސިމްޓޮމެޓިކް އިންފެކްޝަން އޭ ކިޔާ އެއްޗަކީ ނެތް އެއްޗެއްކަން ސާބިތުކޮށްދީފަ އެވެ.
އެސިމްޓޮމެޓިކް އިންފެކްޝަން އަކީ ނެތް އެއްޗެކެވެ. ޓެސްޓުން ޕޮޒިޓިވް ވިޔަސް ބަލީގެ ޢަލާމާތްތައް ނުފެންނަ މީހުންނަކީ ބަލި ފަތުރާ ބައެއް ނޫން ކަމުގައި ވޫހާންގެ 10 މިލިއަން އަށް ގާތްކުރާ އާބާދީގެ މައްޗަށް ހެދި ތަހުލީލުންވަނީ ދައްކާފަ އެވެ. ޢަލާމާތް ނުފެންނަ މީހެއްގެ ކިބައިން ކޮވިޑް-19 އެއްމެ މީހަކަށްވެސް ޖެހިފައިނުވާ ކަމުގައި މިދިރާސާގައިވަނީ ބަޔާންކޮށްފަ އެވެ.[20]
“The citywide nucleic acid screening of SARS-CoV-2 infection in Wuhan recruited nearly 10 million people, and found no newly confirmed cases with COVID-19. The detection rate of asymptomatic positive cases was very low, AND THERE WAS NO EVIDENCE OF TRANSMISSION FROM ASYMPTOMATIC POSITIVE PERSONS TO TRACED CLOSE CONTACTS. THERE WERE NO ASYMPTOMATIC POSITIVE CASES IN 96.4% OF THE RESIDENTIAL COMMUNITIES.”
އަދި މި ޕޭޕަރުގައި ބުނެފައިވަނީ ޕީސީއާރް ޕޮޒިޓިވް ކޭސެސް ތަކުގައި “ވިއަބަލް (މަސައްކަތްކުރާ) ވައިރަސް” ފެނިފައިނުވާ ކަމުގަ އެވެ.
no “viable virus” in positive cases detected in this study.[21]
މާސް ޓެސްޓުކުރުންތައް ހުއްޓާލައި، ޢަލާމާތްތައް ނުފެންނަ މީހުން ކަރަންޓީނުކޮށް ބަންދުކުރުން ހުއްޓާލަން ނުވޭތޯ އެވެ؟ ބަލީގެ ޢަލާމާތެއް ނުފެންނަ މީހަކީ ޞިއްޙަތު ސަލާމަތުން ހުރި މީހެކެވެ. މީގެ މާނަ އަކީ ޢަލާމާތެއް ނުފެންނަ މީހެއްގެ މައްޗަށް މީހުން ބިރުގަނެ އުޅެން ނުޖެހޭ ކަމެވެ. އަދި މި ޓެސްޓަށް ޕޮޒިޓިވް ވުމަކީ އެމީހަކު ބަލި މީހެއްގެ ގޮތުގައި ކަނޑައަޅައި ބިރު ގަންނަވަން ޖެހޭ ކަމެއް ނޫން ކަމެވެ.
“އެމީހުން އަދި (ކޮވިޑް-19) ވައިރަސް އައިޑެންޓިފައިކޮށް ހޯދާފައެއް ނެތް. އެމީހުން ޓެސްޓު އެކުރަނީ ކޮން އެއްޗަކަށް ތޯ؟ އެކުރަނީ ޑީއެންއޭ ( އާރުއެންއޭ ) ސީކްއެންސްތަކުގެ ފްރެގްމެންޓް ތަކަކަށް. މީހުންނަށް ފަހުމްވާން ޖެހޭ، މި މީހުން ކޮރޯނާ ވައިރަސް އައިސޮލޭޓް ކޮށް، ޕިއުރިފައި ކޮށް، ރީޕްރޮޑިއުސް ކޮށް، އެ ވައިރަސް އެއް ޖަނަވާރުތައް ބޭނުންކޮށް ބަލިޖައްސާ އެއްޗެއްތޯ ޓެސްޓު ކޮށްފައިނުވޭ. ވައިރަސް އެއް ހޯދޭނީ ވައިރަސްއެއް އައިސޮލޭޓް ކޮށްގެން. އޭގެ ވަށައިގެންވާ ދައުރުކުރާ އެހެން ބޭކާރު އެއްޗެހިން އެ ސާފުކޮށް ޕިއުރިފައި ކޮށްގެން. އަދި އޭތި އާލާކޮށްގެން، އެއިން އާލާކުރެވުނީ ކުނިބުނި ނޫންކަން ޔަޤީންކޮށްގެން. އަދި ތިބުނާ ޢަލާމާތްތައް ފެންނަނީ އެ ވައިރަސްގެ ސަބަބުން ކަން ޓެސްޓުކޮށް ތަޙުލީލުކޮށްގެން. އެމީހުންނެއް މިކަމެއް ނުކުރޭ. އެހެންކަމުން، ގޭގޭގެ ދޮރުން-ދޮރަށް ގޮސް ސިފައިން ބޭނުންކޮށް މި ކުރަނީ ކޮން ޓެސްޓެއް؟ އެމީހުން ޓެސްޓު އެކުރަނީ އަހަރެމެން އަޅުވެތިކޮށް ކޮންޓްރޯލް ކުރެވޭނީ ކިހާވަރަކަށް ތޯ ބަލަން؟”
11 ނޮވެންމަރ 20202:
Most importantly, the judges ruled that a single positive PCR test cannot be used as an effective diagnosis of infection.
Citing Jaafar et al. 2020 : “At Ct = 35, the value we used to report a positive result for PCR, <3% of cultures are positive.” [22]
Portuguese Court Rules PCR Tests “Unreliable” & Quarantines “Unlawful” https://off-guardian.org/2020/11/20/portuguese-court-rules-pcr-tests-unreliable-quarantines-unlawful
The court stated, the test’s reliability depends on the number of cycles used and the viral load present. Citing Jaafar et al. 2020, the court concludes that
“if someone is tested by PCR as positive when a threshold of 35 cycles or higher is used (as is the rule in most laboratories in Europe and the US), the probability that said person is infected is less than 3%, and the probability that said result is a false positive is 97%.”
The court further notes that the cycle threshold used for the PCR tests currently being made in Portugal is unknown.
The threshold cycles used in PCR tests in India is between 37 and 40, which makes the reliability of the PCR test less than 3% and the false positive rate as high as 97%.
000000000000000000000000000000000
In a recent decision, dated November 11, 2020, a Portuguese appeal court ruled against the Azores Regional Health Authority concerning a lower court decision to declare unlawful the quarantining of four persons. Of these, one had tested positive for Covid using a PCR test; the other three were deemed to have undergone a high risk of exposure. Consequently, the Regional Health Authority decided that all four were infectious and a health hazard, which required that they go into isolation. The lower court had ruled against the Health Authority, and the appeal court upheld that ruling with arguments that explicitly endorse the scientific case for the lack of reliability of the PCR tests (e.g., as extensively explained in Lockdown Skeptics by Dr. Mike Yeadon, Dr. Clare Craig and others).
The court’s ruling is a long text. I provide below a summary of the key passage.
The court’s main points are as follows:
- A medical diagnosis is a medical act that only a physician is legally qualified to undertake and for which such physician will be solely and entirely responsible. No other person or institution, including government agencies or the courts, has such an authority. It is not up to the Azores Regional Health Authority to declare someone ill, or a health hazard. Only a physician can do that. No one can be declared ill or a health hazard by decree or law, nor as the automatic, administrative consequence of the outcome of a laboratory test, no matter which.
- From the above, the court concludes that “if carried out with no prior medical observation of the patient, with no participation of a physician certified by the Ordem dos Médicos who would have assessed symptoms and requested the tests/exams deemed necessary, any act of diagnosis, or any act of public health vigilance (such as determining whether a viral infection or a high risk of exposure exist, which the aforementioned concepts subsume) will violate [a number of laws and regulations] and may configure a crime of usurpação de funções [unlawful practice of a profession] in the case said acts are carried out or dictated by someone devoid of the capacity to do so, i.e., by someone who is not a certified physician [to practice medicine in Portugal a degree is not enough, you need to be accepted as qualified to practice medicine by undergoing examination with the Ordem dos Médicos, roughly our equivalent of the UK’s Royal College of Physicians].”
- In addition, the court rules that the Azores Health Authority violated article 6 of the Universal Declaration on Bioethics and Human Rights, as it failed to provide evidence that the informed consent mandated by said Declaration had been given by the PCR-tested persons who had complained against the forced quarantine measures imposed on them.
- From the facts presented to the court, it concluded that no evidentiary proof or even indication existed that the four persons in question had been seen by a doctor, either before or after undertaking the test.
The above would suffice to deem the forced quarantine of the four persons unlawful. The court thought it necessary, however, to add some very interesting considerations about the PCR tests:
- “Based on the currently available scientific evidence this test [the RT-PCR test] is in and of itself unable to determine beyond reasonable doubt that positivity in fact corresponds to infection by the SARS-CoV-2 virus, for several reasons, among which two are paramount (to which one would need to add the issue of the gold standard, which, due to that issue’s specificity, will not be considered here): the test’s reliability depends on the number of cycles used; the test’s reliability depends on the viral load present.”
- Citing Jaafar et al. (2020;), the court concludes that “if someone is tested by PCR as positive when a threshold of 35 cycles or higher is used (as is the rule in most laboratories in Europe and the US), the probability that said person is infected is <3%, and the probability that said result is a false positive is 97%.” The court further notes that the cycle threshold used for the PCR tests currently being made in Portugal is unknown [N.B. – I know from acquaintances that in at least some Portuguese labs the threshold is 35 cycles].
- Citing Surkova et al. (2020)), the court further states that any diagnostic test must be interpreted in the context of the actual probability of disease as assessed prior to the undertaking of the test itself, and expresses the opinion that “in the current epidemiological landscape of the United Kingdom, the likelihood is increasing that Covid 19 tests are returning false positives, with major implications for individuals, the health system and society.”
The court’s summary of the case to rule against the Regional Health Authority’s appeal reads as follows:
- “Given how much scientific doubt exists — as voiced by experts, i.e., those who matter — about the reliability of the PCR tests, given the lack of information concerning the tests’ analytical parameters, and in the absence of a physician’s diagnosis supporting the existence of infection or risk, there is no way this court would ever be able to determine whether C was indeed a carrier of the SARS-CoV-2 virus, or whether A, B and D had been at a high risk of exposure to it.”
I anticipate this ruling to have massive legal implications in my country. Note that it comes in the back of a previous ruling by the Constitutional Court, our highest court, declaring as an unlawful deprivation of liberty a decision by the Regional Government of the Azores to force into a 14-day quarantine every passenger landing in an airport of the territory.
PCR data evaluated as positive after a Ct value of 35 cycles are completely unreliable.
Citing Jaafar et al. 2020 : “At Ct = 35, the value we used to report a positive result for PCR, <3% of cultures are positive.” [23]
In other words, there was no successful virus isolation of SARS-CoV-2 at those high Ct values.
Further, scientific studies show that only non-infectious (dead) viruses are detected with Ct values of 35 [22].[24]
4 ވަނަ މައްސަލަ
(4) Biomolecular validations: The fact that these PCR products have not been validated at molecular level is another striking error of the protocol, making any test based upon it useless as a specific diagnostic tool to identify the SARS-CoV-2 virus.
To determine whether the amplified products are indeed SARS-CoV-2 genes, biomolecular validation of amplified PCR products is essential. For a diagnostic test, this validation is an absolute must.
Validation of PCR products should be performed by either running the PCR product in a 1% agarose-EtBr gel together with a size indicator (DNA ruler or DNA ladder) so that the size of the product can be estimated. The size must correspond to the calculated size of the amplification product. But it is even better to sequence the amplification product. The latter will give 100% certainty about the identity of the amplification product. Without molecular validation one can not be sure about the identity of the amplified PCR products. Considering the severe design errors described earlier, the amplified PCR products can be anything.
Also not mentioned in the Corman-Drosten paper is the case of small fragments of qPCR (around 100bp): It could be either 1,5% agarose gel or even an acrylamide gel.
8. The Corman-Drosten paper was not peer-reviewed
Before formal publication in a scholarly journal, scientific and medical articles are traditionally certified by “peer review.” In this process, the journal’s editors take advice from various experts (“referees”) who have assessed the paper and may identify weaknesses in its assumptions, methods, and conclusions. Typically a journal will only publish an article once the editors are satisfied that the authors have addressed referees’ concerns and that the data presented supports the conclusions drawn in the paper.” This process is as well described for Eurosurveillance [16].
The Corman-Drosten paper was submitted to Eurosurveillance on January 21st 2020 and accepted for publication on January 22nd 2020. On January 23rd 2020 the paper was online. On January 13th 2020 version 1-0 of the protocol was published at the official WHO website [17], updated on January 17th 2020 as document version 2-1 [18], even before the Corman-Drosten paper was published on January 23rd at Eurosurveillance.
Normally, peer review is a time-consuming process since at least two experts from the field have to critically read and comment on the submitted paper. In our opinion, this paper was not peer-reviewed. Twenty-four hours are simply not enough to carry out a thorough peer review. Our conclusion is supported by the fact that a tremendous number of very serious design flaws were found by us, which make the PCR test completely unsuitable as a diagnostic tool to identify the SARS-CoV-2 virus. Any molecular biologist familiar with RT-PCR design would have easily observed the grave errors present in the Corman-Drosten paper before the actual review process. We asked Eurosurveillance on October 26th 2020 to send us a copy of the peer review report. To date, we have not received this report and in a letter dated November 18th 2020, the ECDC as host for Eurosurveillance declined to provide access without providing substantial scientific reasons for their decision. On the contrary, they write that “disclosure would undermine the purpose of scientific investigations.” [24].
SUMMARY CATALOGUE OF ERRORS FOUND IN THE PAPER
The Corman-Drosten paper contains the following specific errors:
1. There exists no specified reason to use these extremely high concentrations of primers in this protocol. The described concentrations lead to increased nonspecific bindings and PCR product amplifications, making the test unsuitable as a specific diagnostic tool to identify the SARS-CoV-2 virus.
2. Six unspecified wobbly positions will introduce an enormous variability in the real world laboratory implementations of this test; the confusing nonspecific description in the Corman-Drosten paper is not suitable as a Standard Operational Protocol making the test unsuitable as a specific diagnostic tool to identify the SARS-CoV-2 virus.
3. The test cannot discriminate between the whole virus and viral fragments. Therefore, the test cannot be used as a diagnostic for intact (infectious) viruses, making the test unsuitable as a specific diagnostic tool to identify the SARS-CoV-2 virus and make inferences about the presence of an infection.
4. A difference of 10° C with respect to the annealing temperature Tm for primer pair1 (RdRp_SARSr_F and RdRp_SARSr_R) also makes the test unsuitable as a specific diagnostic tool to identify the SARS-CoV-2 virus.
5. A severe error is the omission of a Ct value at which a sample is considered positive and negative. This Ct value is also not found in follow-up submissions making the test unsuitable as a specific diagnostic tool to identify the SARS-CoV-2 virus.
6. The PCR products have not been validated at the molecular level. This fact makes the protocol useless as a specific diagnostic tool to identify the SARS-CoV-2 virus.
7. The PCR test contains neither a unique positive control to evaluate its specificity for SARS-CoV-2 nor a negative control to exclude the presence of other coronaviruses, making the test unsuitable as a specific diagnostic tool to identify the SARS-CoV-2 virus.
8. The test design in the Corman-Drosten paper is so vague and flawed that one can go in dozens of different directions; nothing is standardized and there is no SOP. This highly questions the scientific validity of the test and makes it unsuitable as a specific diagnostic tool to identify the SARS-CoV-2 virus.
9. Most likely, the Corman-Drosten paper was not peer-reviewed making the test unsuitable as a specific diagnostic tool to identify the SARS-CoV-2 virus.
10. We find severe conflicts of interest for at least four authors, in addition to the fact that two of the authors of the Corman-Drosten paper (Christian Drosten and Chantal Reusken) are members of the editorial board of Eurosurveillance. A conflict of interest was added on July 29 2020 (Olfert Landt is CEO of TIB-Molbiol; Marco Kaiser is senior researcher at GenExpress and serves as scientific advisor for TIB-Molbiol), that was not declared in the original version (and still is missing in the PubMed version); TIB-Molbiol is the company which was “the first” to produce PCR kits (Light Mix) based on the protocol published in the Corman-Drosten manuscript, and according to their own words, they distributed these PCR-test kits before the publication was even submitted [20]; further, Victor Corman & Christian Drosten failed to mention their second affiliation: the commercial test laboratory “Labor Berlin”. Both are responsible for the virus diagnostics there [21] and the company operates in the realm of real time PCR-testing
[1] Covid-19: politicisation, “corruption,” and suppression of science https://www.bmj.com/content/371/bmj.m4425
[2] China has made major progress on air pollution. Wuhan protests show there’s still a long way to go https://edition.cnn.com/2019/07/10/asia/china-wuhan-pollution-problems-intl-hnk/index.html
[3] Wuhan protests: Incinerator plan sparks mass unrest https://www.bbc.com/news/blogs-china-blog-48904350
[4] Return to Wuhan: What Life Is Like One Year Later | NBC Nightly News https://www.youtube.com/watch?v=YbSdG2imqEM
[5] Why Most Published Research Findings Are False https://journals.plos.org/plosmedicine/article?id=10.1371/journal.pmed.0020124
[6] Peng Zhou, el at. Discovery of a novel coronavirus associated with the recent pneumonia outbreak in humans and its potential bat origin. https://www.biorxiv.org/content/10.1101/2020.01.22.914952v1
[7] A Novel Coronavirus from Patients with Pneumonia in China, 2019 https://www.nejm.org/doi/full/10.1056/NEJMoa2001017
[8] Discussion, Na Zhu, N Engl J Med 2020; 382:727-733
[9] Rivers, T. M. Virus and Koch’s Postulates.J.Bacteriol.33, 1-12 (1937)
[10] Identification of a novel coronavirus causing severe pneumonia in human: a descriptive study https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7147275
[11] Detection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR https://www.eurosurveillance.org/content/10.2807/1560-7917.ES.2020.25.3.2000045
[12] Detection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6988269
[13] Ten Fatal Errors: Scientists Attack Paper That Established Global PCR Driven Lockdown
By Celia Farber -December 3, 2020 https://uncoverdc.com/2020/12/03/ten-fatal-errors-scientists-attack-paper-that-established-global-pcr-driven-lockdown
[14] P. Borger (MSc, PhD) is an expert in molecular genetics. He is a science writer and author. Coleader of the Retraction Initiative of the Corman-Drosten paper. https://twitter.com/borgerpieter
[15] CDC 2019-Novel Coronavirus (2019-nCoV) Real-Time RT-PCR Diagnostic Panel https://www.fda.gov/media/134922/download
[16] June 8, 2020 – Anthony Fauci, MD, on COVID-19 Vaccines, Schools, and Larry Kramer https://jamanetwork.com/journals/jama/fullarticle/2767208
[17] July 16, 2020 – TWiV 641: COVID-19 with Dr. Anthony Fauci https://twitter.com/vegsource/status/1322285840291147776?s=20
[18] 28 September 2020 – Correlation Between 3790 Quantitative Polymerase Chain Reaction–Positives Samples and Positive Cell Cultures, Including 1941 Severe Acute Respiratory Syndrome Coronavirus 2 Isolates https://academic.oup.com/cid/advance-article/doi/10.1093/cid/ciaa1491/5912603
[19] Infection fatality rate of COVID-19 inferred from seroprevalence data https://www.who.int/bulletin/online_first/BLT.20.265892.pdf
[20] Post-lockdown SARS-CoV-2 nucleic acid screening in nearly ten million residents of Wuhan, China https://www.nature.com/articles/s41467-020-19802-w
[21] 20 November 2020، Post-lockdown SARS-CoV-2 nucleic acid screening in nearly ten million residents of Wuhan, China https://www.nature.com/articles/s41467-020-19802-w
[22] Jafaar et al., Correlation Between 3790 Quantitative Polymerase Chain Reaction–Positives Samples and Positive Cell Cultures, Including 1941 Severe Acute Respiratory Syndrome Coronavirus 2 Isolates. https://academic.oup.com/cid/advance-article/doi/10.1093/cid/ciaa1491/5912603
[23] Jafaar et al., Correlation Between 3790 Quantitative Polymerase Chain Reaction–Positives Samples and Positive Cell Cultures, Including 1941 Severe Acute Respiratory Syndrome Coronavirus 2 Isolates. https://academic.oup.com/cid/advance-article/doi/10.1093/cid/ciaa1491/5912603
[24] Tom Jefferson, Elizabeth Spencer, Jon Brassey, Carl Heneghan Viral cultures for COVID-
19 infectivity assessment. Systematic review. Systematic review doi:
https://doi.org/10.1101/2020.08.04.20167932 https://www.medrxiv.org/content/10.1101/2020.08.04.20167932v4
